Scapula Fractures Explained By Dr. Faheem Kotekar: What Every Orthopedic Resident Should Know
Scapular fractures are not something we see every day in practice. In fact, they form a very small percentage of overall fractures. But whenever a scapula is fractured, it usually tells a bigger story — one of high-energy trauma and multiple associated injuries. That is why scapular fractures deserve attention far beyond just the bone itself. This blog […]
Interbody Fusion in Lumbar Canal Stenosis- A Practical Surgical Approach Explained by Dr. Jitesh Manghwani
Lumbar canal stenosis is one of the most common causes of back pain, radiculopathy, and neurogenic claudication in adults. When conservative treatment fails, surgical decompression with interbody fusion becomes the definitive solution. But one of the most confusing aspects for residents and young surgeons is choosing the right surgical approach — anterior, lateral, or posterior. Here, in this […]
DNB Theory Questions Explained: Arthroplasty & AVN of Femoral Head By Dr. Vishal Huggi
DNB theory exams often look intimidating, but most questions are actually straightforward scoring opportunities—if you know how much to write and how to structure your answer. In this session, Dr. Vishal Huggi breaks down two commonly asked 3–5 mark questions from Orthopedics in a very practical, exam-focused way. Let’s understand both questions exactly the way […]
13th CO Trauma Foundation Course(Mumbai): A Must-Join Program for Orthopedics Residents
If you missed the opportunity to be a part of the 12th CO Trauma Foundation Course, here’s some good news — the 13th edition is coming soon, and you still have the chance to join one of the most structured and concept-driven trauma courses in orthopedics. For orthopedics residents, MS residents, and early-career orthopedic surgeons, […]
Confused about choosing Orthopedics as a Branch? Honest Answers for Students
Clearing NEET PG feels like winning a battle, but counselling quickly reminds you that the real challenge is still ahead — choosing the right branch. With opinions flying in from seniors, relatives, social media, and coaching mentors, confusion is almost guaranteed. If orthopedics is on your list, you’re probably asking yourself the same questions many […]
NEET SS 2025: One Month. One Chance. One Platform That Changes Everything — Conceptual Orthopedics

With the NEET SS 2025 clock ticking down to the final month, every single minute is currency. You already know this isn’t just another test. It’s a notoriously difficult beast, famous for its unpredictable, clinical-heavy questions and a relentless focus on real-world surgical application. If you’re locked into Orthopedics NEET SS, you’re wrestling with brutal […]
Understanding Degenerative Cervical Myelopathy: Causes, Classifications & Clinical Insights

Degenerative Cervical Myelopathy (DCM) falls under a broad umbrella of conditions affecting the spinal cord. Within this umbrella lies a subset of myelopathy caused by bulging or herniated discs, vertebral deformities, osteophytes, facet joint arthropathies, hypermobility, instability, and spondylolisthesis. On the other side of this umbrella are ligamentous pathologies like OPLL (Ossified Posterior Longitudinal Ligament) […]
Understanding Clubfoot: Clinical Features, Diagnosis, and Evaluation in Newborns
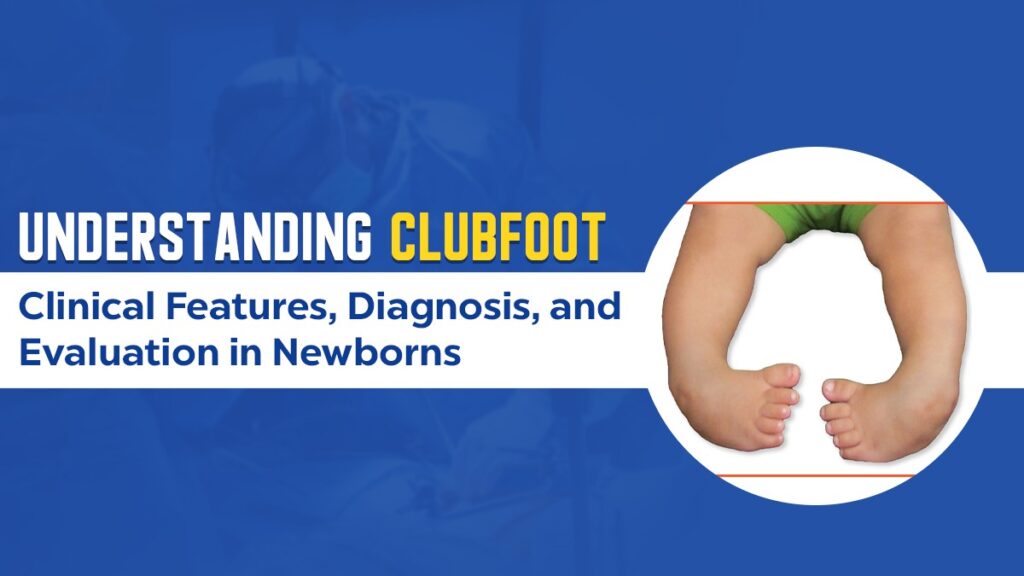
Clubfoot, also called Congenital Talipes Equinovarus (CTEV), is considered one of the most common inherited lower limb deformities, which is generally seen in newborns. It is a structural deformity that was present at the time of birth, but if it is not recognized and treated appropriately, it can lead to lifelong disability. For taking concern […]
Decoding Adhesive Capsulitis: Dr. Harpreet Singh’s Step-by-Step Guide to Clinical Mastery

If you’re asked to discuss or diagnose a case of adhesive capsulitis (frozen shoulder) in your exams or wards, there’s a certain structure that can make all the difference. Dr. Harpreet Singh, known for his clear, concept-driven teaching, explains exactly how to approach such cases — from history taking to examination and management — just […]
Elevate Your Orthopedic Skills with Conceptual Orthopedics Upcoming Courses
A Chance to Enhance Your Knowledge & Skills in the Field of Orthopedics Are you a budding orthopedic professional eager to take your expertise to the next level? Conceptual Orthopedics invites you to be a part of its highly anticipated signature programs. A series of live events and hands-on workshops is held across India. While […]